Contents
- Healthcare Infrastructure
- The Three-Tiered Structure of the District
- Medical Education & Research
- Radhakisan Toshniwal Ayurved Mahavidyalaya
- Government Medical College
- Age Old Practices & Remedies
- Public Health Challenges in the District Through Time
- COVID Stories
- Sanitation | Public Toilets & Cleanliness
- Graphs
- Healthcare Facilities and Services
- A. Public and Govt-Aided Medical Facilities
- B. Private Healthcare Facilities
- C. Approved vs Working Anganwadi
- D. Anganwadi Building Types
- E. Anganwadi Workers
- F. Patients in In-Patients Department
- G. Patients in Outpatients Department
- H. Outpatient-to-Inpatient Ratio
- I. Patients Treated in Public Facilities
- J. Operations Conducted
- K. Hysterectomies Performed
- L. Share of Households with Access to Health Amenities
- Morbidity and Mortality
- A. Reported Deaths
- B. Cause of Death
- C. Reported Child and Infant Deaths
- D. Reported Infant Deaths
- E. Select Causes of Infant Death
- F. Number of Children Diseased
- G. Population with High Blood Sugar
- H. Population with Very High Blood Sugar
- I. Population with Mildly Elevated Blood Pressure
- J. Population with Moderately or Severely High Hypertension
- K. Women Examined for Cancer
- L. Alcohol and Tobacco Consumption
- Maternal and Newborn Health
- A. Reported Deliveries
- B. Institutional Births: Public vs Private
- C. Home Births: Skilled vs Non-Skilled Attendants
- D. Live Birth Rate
- E. Still Birth Rate
- F. Maternal Deaths
- G. Registered Births
- H. C-section Deliveries: Public vs Private
- I. Institutional Deliveries through C-Section
- J. Deliveries through C-Section: Public vs Private Facilities
- K. Reported Abortions
- L. Medical Terminations of Pregnancy: Public vs Private
- M. MTPs in Public Institutions before and after 12 Weeks
- N. Average Out of Pocket Expenditure per Delivery in Public Health Facilities
- O. Registrations for Antenatal Care
- P. Antenatal Care Registrations Done in First Trimester
- Q. Iron Folic Acid Consumption Among Pregnant Women
- R. Access to Postnatal Care from Health Personnel Within 2 Days of Delivery
- S. Children Breastfed within One Hour of Birth
- T. Children (6-23 months) Receiving an Adequate Diet
- U. Sex Ratio at Birth
- V. Births Registered with Civil Authority
- W. Institutional Deliveries through C-section
- X. C-section Deliveries: Public vs Private
- Family Planning
- A. Population Using Family Planning Methods
- B. Usage Rate of Select Family Planning Methods
- C. Sterilizations Conducted (Public vs Private Facilities)
- D. Vasectomies
- E. Tubectomies
- F. Contraceptives Distributed
- G. IUD Insertions: Public vs Private
- H. Female Sterilization Rate
- I. Women’s Unmet Need for Family Planning
- J. Fertile Couples in Family Welfare Programs
- K. Family Welfare Centers
- L. Progress of Family Welfare Programs
- Immunization
- A. Vaccinations under the Maternal and Childcare Program
- B. Infants Given the Oral Polio Vaccine
- C. Infants Given the Bacillus Calmette Guerin (BCG) Vaccine
- D. Infants Given Hepatitis Vaccine (Birth Dose)
- E. Infants Given the Pentavalent Vaccines
- F. Infants Given the Measles or Measles Rubella Vaccines
- G. Infants Given the Rotavirus Vaccines
- H. Fully Immunized Children
- I. Adverse Effects of Immunization
- J. Percentage of Children Fully Immunized
- K. Vaccination Rate (Children Aged 12 to 23 months)
- L. Children Primarily Vaccinated in (Public vs Private Health Facilities)
- Nutrition
- A. Children with Nutritional Deficits or Excess
- B. Population Overweight or Obese
- C. Population with Low BMI
- D. Prevalence of Anaemia
- E. Moderately Anaemic Women
- F. Women with Severe Anaemia being Treated at an Institution
- G. Malnourishment Among Infants in Anganwadis
- Sources
AKOLA
Health
Last updated on 4 November 2025. Help us improve the information on this page by clicking on suggest edits or writing to us.
Akola’s healthcare landscape, like many other regions across India, is shaped by a mix of indigenous and Western medical practices. For centuries, indigenous knowledge and treatments provided by practitioners such as hakims and vaidyas have formed the foundation of healthcare in the region. Locals note that, as a large portion of Akola’s population resides in rural areas, the district’s medical practices remain deeply rooted in age-old traditions. Hence, even though Western medicinal facilities are growing within the district of Akola, the tradition of nuskes and parasbaugs (परसबाग) remains alive in every nook and corner of local households.
Healthcare Infrastructure
Much like other regions in India, Akola’s healthcare infrastructure follows a multi-tiered system that involves both public and private sectors. Currently, the public healthcare system is tiered into primary, secondary, and tertiary levels. Primary care is provided through Sub Centres and Primary Health Centres (PHCs), while secondary care is managed by Community Health Centres (CHCs) and Sub-District hospitals. Tertiary care, the highest level, includes Medical Colleges and District Hospitals. This system has evolved and been refined over time, influenced by national healthcare reforms.
The Three-Tiered Structure of the District
Akola’s formal healthcare infrastructure, like much of India, has its origins in the colonial era, which laid the groundwork for the system in place today. One of the earliest such institutions was the District Hospital of Akola, established in 1927. A network of municipal hospitals and dispensaries were formed across the region after this.
Over time this landscape began to change over time. The public health infrastructure began expanding. In 2002, the Government Medical College and Hospital was founded to expand the district’s capacity for medical education and advanced care. This development was followed by the inauguration of a new super speciality hospital in 2022, built at an investment of approximately 150 crore INR. This facility provides services such as neurology, radiology, and plastic surgery, and accommodates over 200 beds.
Additionally, in the 20th and 21st centuries, private hospitals started to emerge in Akola; with their establishment being driven by trusts, NGOs, and locals themselves.
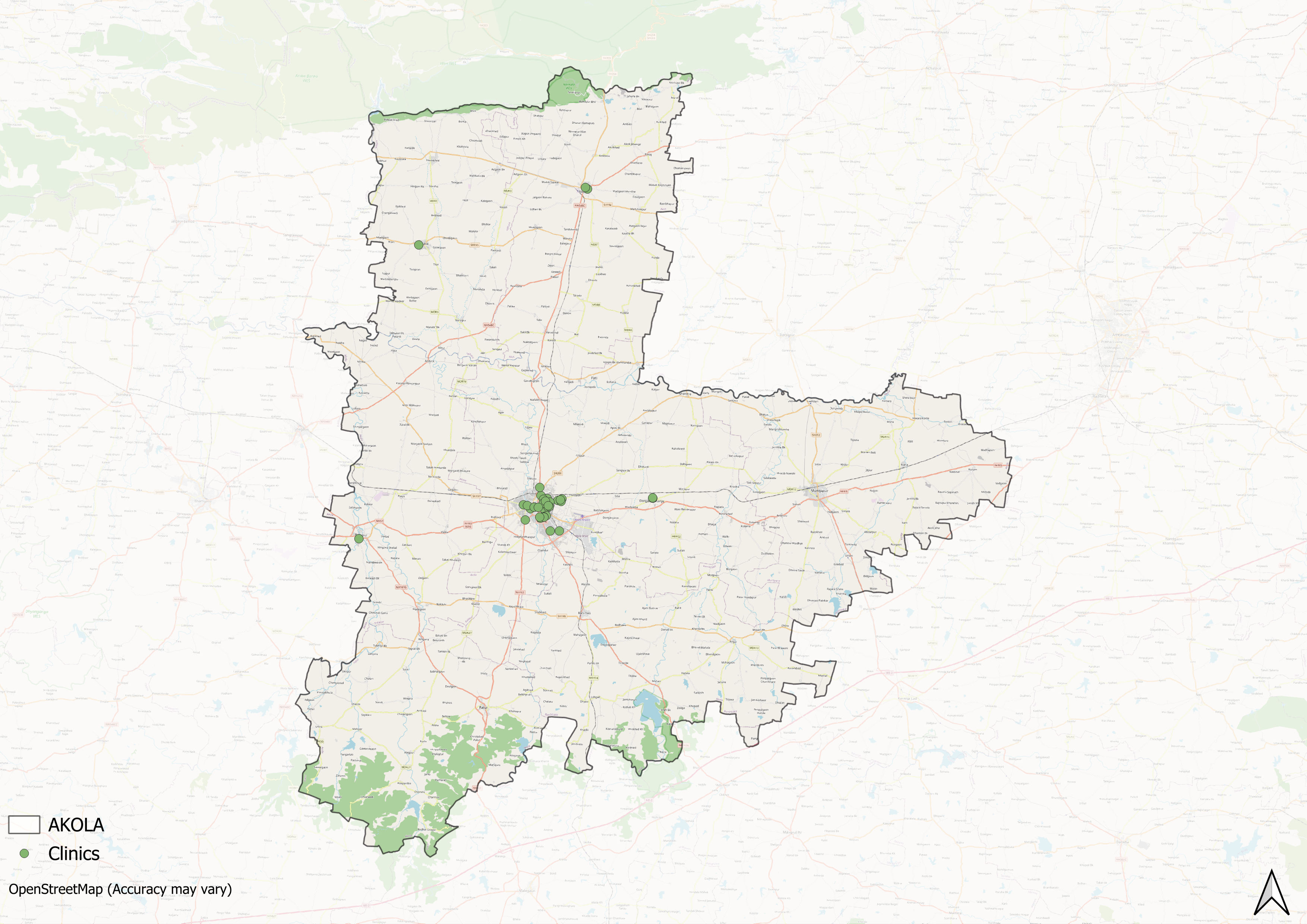
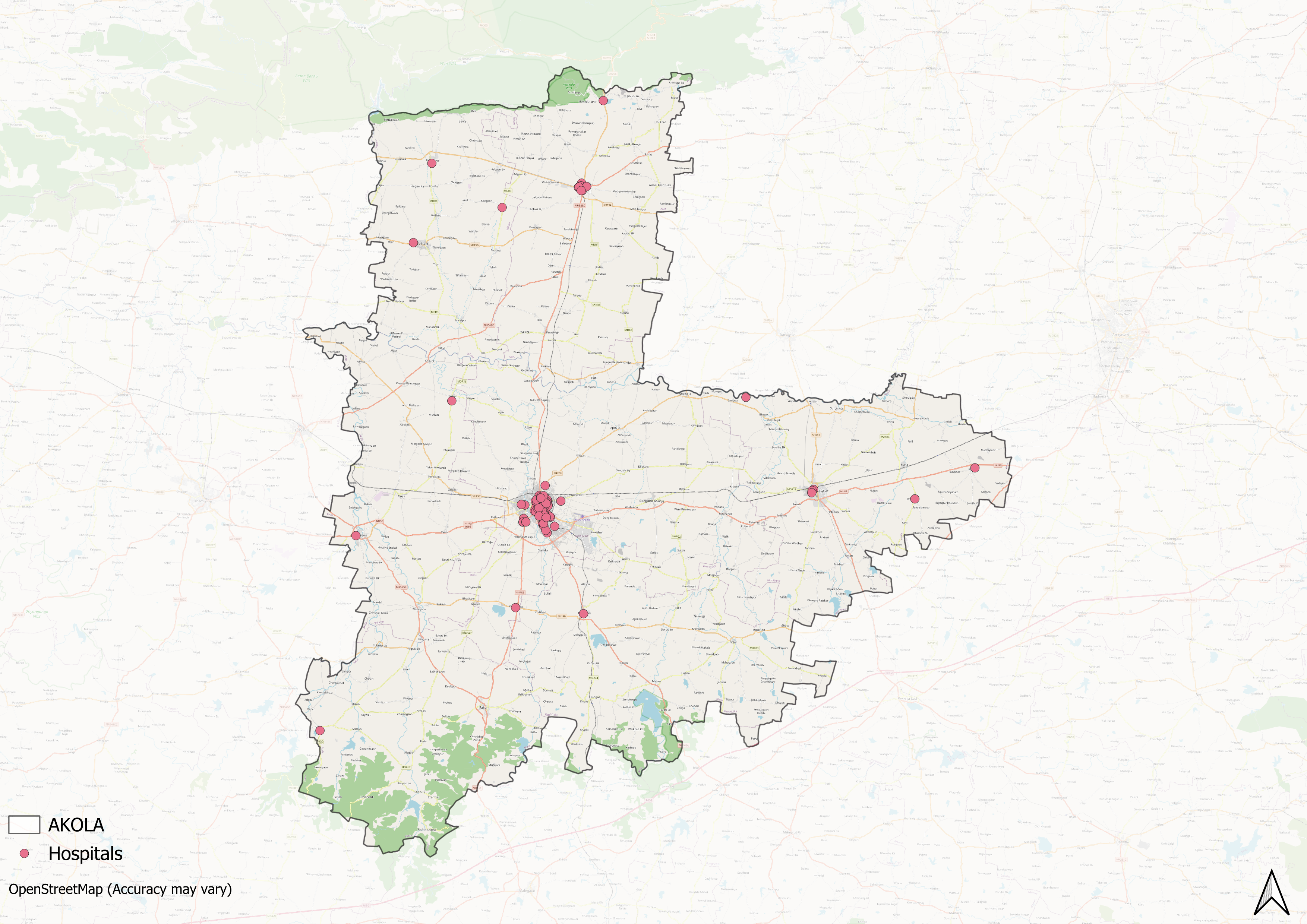
However, similar to broader patterns that can be seen across India, the district’s healthcare infrastructure has developed unevenly across geographic lines. While urban areas experienced substantial growth in private healthcare facilities, rural regions remained predominantly served by government-run hospitals, with fewer private facilities.
Medical Education & Research
Medical education and research are foundational to a district’s healthcare infrastructure. As Mathew Gerge (2023) aptly highlights, medical institutions often serve a “dual purpose,” which includes educating future healthcare professionals and providing healthcare services to the local population. The medical education landscape in Akola spans multiple healthcare traditions such as allopathy, ayurveda, and homeopathy, much in line with India’s pluralistic healthcare traditions.
Radhakisan Toshniwal Ayurved Mahavidyalaya
Radhakisan Toshniwal Ayurved Mahavidyalaya, situated in the Gudhadi area of Akola, was established in 1955 by the Rashtriya Vaidyak Prasarak Mandal. The institute appears to be of much importance as it is regarded to be among the oldest Ayurvedic colleges in the Vidarbha region.
![Main building of Radhakisan Toshniwal Ayurved Mahavidyalaya, established in 1955.[1]](/media/statistic/images/maharashtra/akola/health/main-building-of-radhakisan-toshniwal-ayurved-_FaW5u6z.png)
The college offers undergraduate and postgraduate courses in Ayurveda and includes departments such as Kaumarbhritya (pediatrics) and Panchakarma (detoxification therapies).
Government Medical College
Government Medical College, Akola (GMC Akola) is a government-run medical institution which was established in 2002. It is affiliated with the Maharashtra University of Health Sciences (MUHS), Nashik and offers various undergraduate courses in the field of medicine and allied health sciences.
The college offers the MBBS program with a duration of 5.5 years, which includes a compulsory internship, and has an annual intake capacity of 200 students. Other courses available include General Nursing and Midwifery (GNM), Bachelor of Science in Paramedical Technology (B.Sc. PMT), Diploma in Medical Laboratory Technology (DMLT), and General Duty Assistant (GDA).
Age Old Practices & Remedies
Historically, before the advent of western health care systems or the three-tiered healthcare infrastructure that exists today, people in the district relied and made use of indigenous knowledge and medicine for their well being. When it comes to healthcare, India, for long has been characterized by a pluralistic health tradition. Among the many medicine systems that have a long history in India and in Akola, as locals say, is Ayurveda and Unani. The use of ayurvedic and unani systems of medicines are prevalent in the district.

Perhaps one of the significant yet frequently overlooked aspects of healthcare traditions includes the role of age-old practices and home-based remedies. In India, as many say, indigenous knowledge and household remedies have for long formed the basis of many family healthcare practices. These local remedies and healing methods have persisted through time through intergenerational transmission.
In Akola, locals recall how, in the past, suinis (traditional birth attendants) and elderly women within families often took charge of treating ailments related to gynecology and childbirth. The remedies and medicines they prepared were commonly referred to as ajibaicha batwa (a term that literally means, “grandmother’s pouch.”)
In many homes across Akola, it is still common to find small gardens and aangans where vegetables and medicinal plants grow side by side. Plants such as Tridax (कंबरमोडी,, Kambarmodi), Momordica (कारले, Karle), and Vasaka (अडुळसा, Adulsa) are cultivated for their healing properties and form the basis of dadi ke nuskes (which are traditional home remedies for everyday ailments).
For instance, White Rui leaves are boiled in black tea to relieve coughs. Shekane, an oil prepared from soybean or coconut oil combined with white and violet Rui, is used to treat swellings. Kavatha is commonly consumed to reduce pitta dosha (excess heat in the body). Yerand is used to manage rheumatic conditions, while Gulvel is a key ingredient in kadhas brewed to help reduce dengue symptoms.
![Murusheng leaves[2]](/media/statistic/images/maharashtra/akola/health/murusheng-leaves2-7a06e044.jpg)
Local traditions also highlight unique remedies for newborn care. Murdasheng leaves, for example, are traditionally crushed and squeezed against a stone to extract milk-like sap given to newborns, which locals believe helps improve digestion and overall health.
Public Health Challenges in the District Through Time
Epidemics and disease outbreaks have significantly shaped public health outcomes throughout history, creating persistent challenges that communities have continuously sought to overcome. In the case of Akola district, documented historical records indicate several key outbreaks that impacted both the population’s health and mortality rates, particularly in the late 19th century. The district Gazetteer (1910) notes that a “plague first appeared in 1902 and has recurred every year. The chief outbreak in Akola town was in 1905.” Notably, dead rats were presumed to be indicators of a plague ever since.
COVID Stories
More recently, during the COVID-19 pandemic, the strain on the district’s hospitals and daily life was sudden and severe. Its highly contagious nature made it particularly challenging to control, especially in the early stages. Many people stepped up to help in small ways. In Shivnagar, Dimple Kavhane, a local tailor, made and gave away more than 2,000 masks when they were hard to find.
Sanitation | Public Toilets & Cleanliness
Sanitation remains a critical issue that needs urgent attention within the district. Beyond general cleanliness, locals have frequently raised concerns about the lack of accessible public toilets. In urban areas, the Akola Mahanagar Palika has constructed public toilets. They have also started a service that provides mobile toilet vans, which can be booked online for large gatherings and private events such as weddings. However, the maintenance and usability often fall short of local needs.
In rural areas, the Hagandari Mukt Yojana aimed to make villages free of open defecation by requiring Gram Panchayats to build household toilets for families without them. However, the implementation of this initiative at the village level has often been uneven. Many locals in Akola report that toilets built under the scheme lack basic amenities such as running water or doors, making them impractical to use and leaving open defecation widespread.
Graphs
Healthcare Facilities and Services
Morbidity and Mortality
Maternal and Newborn Health
Family Planning
Immunization
Nutrition
Sources
Chokshi, M., Patil, B., Khanna, R., Neogi, S. B., Sharma, J., Paul, V. K., & Zodpey, S. 2016. "Health systems in India." Journal of Perinatology. Vol. 36, Suppl. 3https://pmc.ncbi.nlm.nih.gov/articles/PMC514…
Deshpande, Chaitanya. 2022. "Akola’s Super Specialty Hospital to Start from August 1, but Where’s the Manpower?" The Times of India, Nagpur. 2025.https://timesofindia.indiatimes.com/city/nag…
Gazetteer Department, Government of Maharashtra. 1977. Akola District Gazetteer. Gazetteer Department, Government of Maharashtra, Mumbai.
George, Mathew. 2023. "The Real Purpose of the Medical College." The Hindu, Place.https://www.thehindu.com/opinion/op-ed/the-r…
Government Medical College, Akola. Undergraduate Course.https://gmcakola.in/UGCourse
Munyi, P., & Jonas, M. 2013. "Protecting Traditional Knowledge and Traditional Medicines of Indigenous Peoples through Intellectual Property Rights: Issues, Challenges and Strategies."Vol. 21, no. 2.African Journal of International and Comparative Law.https://www.jstor.org/stable/24675285
Last updated on 4 November 2025. Help us improve the information on this page by clicking on suggest edits or writing to us.