Contents
- Healthcare Infrastructure
- Medical Education & Research
- Government Medical College
- Rajarshi Shahu College of Pharmacy
- Graphs
- Healthcare Facilities and Services
- A. Public and Govt-Aided Medical Facilities
- B. Private Healthcare Facilities
- C. Approved vs Working Anganwadi
- D. Anganwadi Building Types
- E. Anganwadi Workers
- F. Patients in In-Patients Department
- G. Patients in Outpatients Department
- H. Outpatient-to-Inpatient Ratio
- I. Patients Treated in Public Facilities
- J. Operations Conducted
- K. Hysterectomies Performed
- L. Share of Households with Access to Health Amenities
- Morbidity and Mortality
- A. Reported Deaths
- B. Cause of Death
- C. Reported Child and Infant Deaths
- D. Reported Infant Deaths
- E. Select Causes of Infant Death
- F. Number of Children Diseased
- G. Population with High Blood Sugar
- H. Population with Very High Blood Sugar
- I. Population with Mildly Elevated Blood Pressure
- J. Population with Moderately or Severely High Hypertension
- K. Women Examined for Cancer
- L. Alcohol and Tobacco Consumption
- Maternal and Newborn Health
- A. Reported Deliveries
- B. Institutional Births: Public vs Private
- C. Home Births: Skilled vs Non-Skilled Attendants
- D. Live Birth Rate
- E. Still Birth Rate
- F. Maternal Deaths
- G. Registered Births
- H. C-section Deliveries: Public vs Private
- I. Institutional Deliveries through C-Section
- J. Deliveries through C-Section: Public vs Private Facilities
- K. Reported Abortions
- L. Medical Terminations of Pregnancy: Public vs Private
- M. MTPs in Public Institutions before and after 12 Weeks
- N. Average Out of Pocket Expenditure per Delivery in Public Health Facilities
- O. Registrations for Antenatal Care
- P. Antenatal Care Registrations Done in First Trimester
- Q. Iron Folic Acid Consumption Among Pregnant Women
- R. Access to Postnatal Care from Health Personnel Within 2 Days of Delivery
- S. Children Breastfed within One Hour of Birth
- T. Children (6-23 months) Receiving an Adequate Diet
- U. Sex Ratio at Birth
- V. Births Registered with Civil Authority
- W. Institutional Deliveries through C-section
- X. C-section Deliveries: Public vs Private
- Family Planning
- A. Population Using Family Planning Methods
- B. Usage Rate of Select Family Planning Methods
- C. Sterilizations Conducted (Public vs Private Facilities)
- D. Vasectomies
- E. Tubectomies
- F. Contraceptives Distributed
- G. IUD Insertions: Public vs Private
- H. Female Sterilization Rate
- I. Women’s Unmet Need for Family Planning
- J. Fertile Couples in Family Welfare Programs
- K. Family Welfare Centers
- L. Progress of Family Welfare Programs
- Immunization
- A. Vaccinations under the Maternal and Childcare Program
- B. Infants Given the Oral Polio Vaccine
- C. Infants Given the Bacillus Calmette Guerin (BCG) Vaccine
- D. Infants Given Hepatitis Vaccine (Birth Dose)
- E. Infants Given the Pentavalent Vaccines
- F. Infants Given the Measles or Measles Rubella Vaccines
- G. Infants Given the Rotavirus Vaccines
- H. Fully Immunized Children
- I. Adverse Effects of Immunization
- J. Percentage of Children Fully Immunized
- K. Vaccination Rate (Children Aged 12 to 23 months)
- L. Children Primarily Vaccinated in (Public vs Private Health Facilities)
- Nutrition
- A. Children with Nutritional Deficits or Excess
- B. Population Overweight or Obese
- C. Population with Low BMI
- D. Prevalence of Anaemia
- E. Moderately Anaemic Women
- F. Women with Severe Anaemia being Treated at an Institution
- G. Malnourishment Among Infants in Anganwadis
- Sources
BULDHANA
Health
Last updated on 26 July 2025. Help us improve the information on this page by clicking on suggest edits or writing to us.
Buldhana’s healthcare landscape, like many other regions across India, is shaped by a mix of indigenous and Western medical practices. For centuries, indigenous knowledge and treatments provided by practitioners such as hakims and vaidyas have formed the foundation of healthcare in the region. This long-standing relationship between communities and their natural environment played a key role in shaping the district’s early medical traditions. Over time, its landscape has gradually evolved with the introduction and expansion of more specialised medical services.
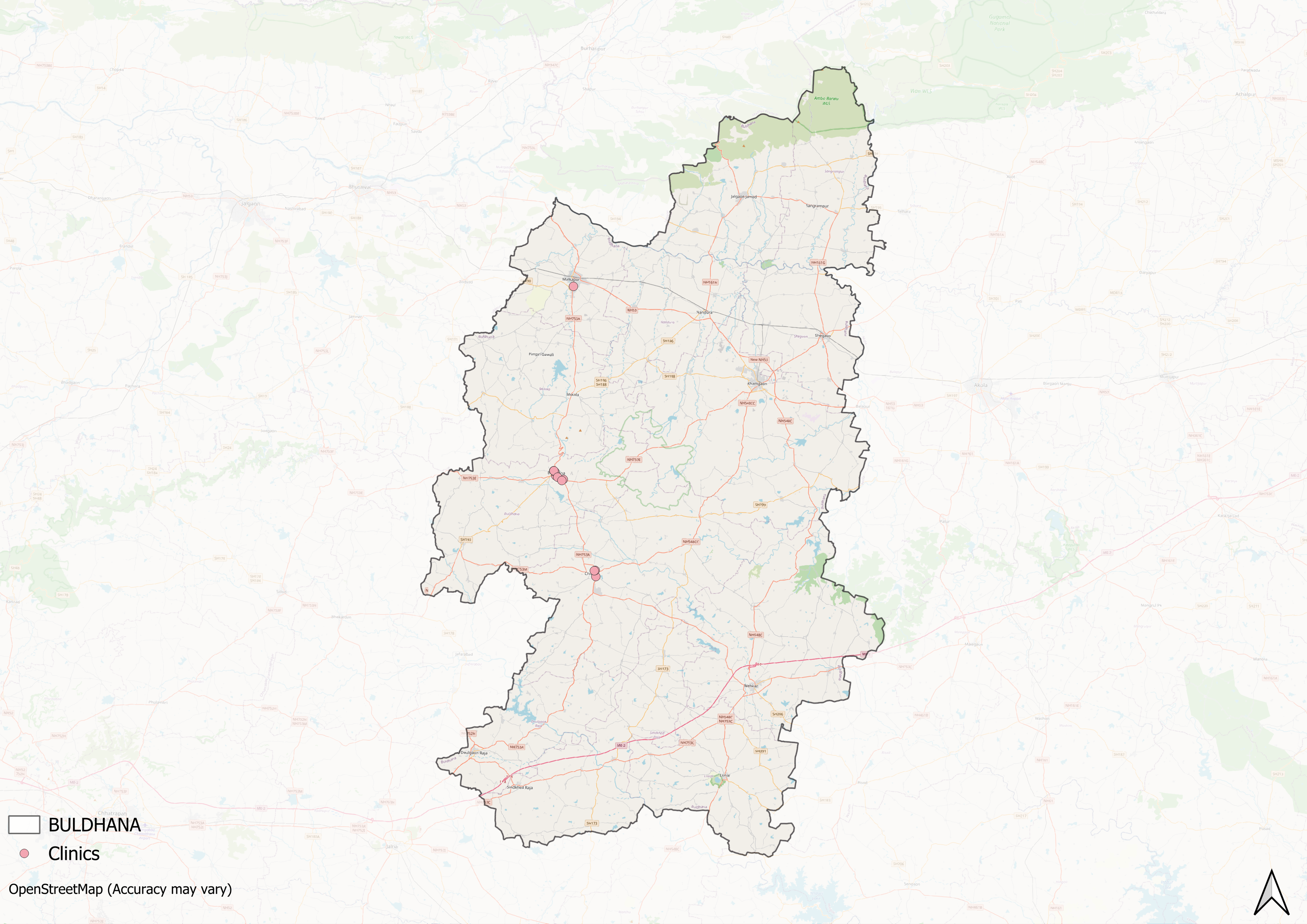
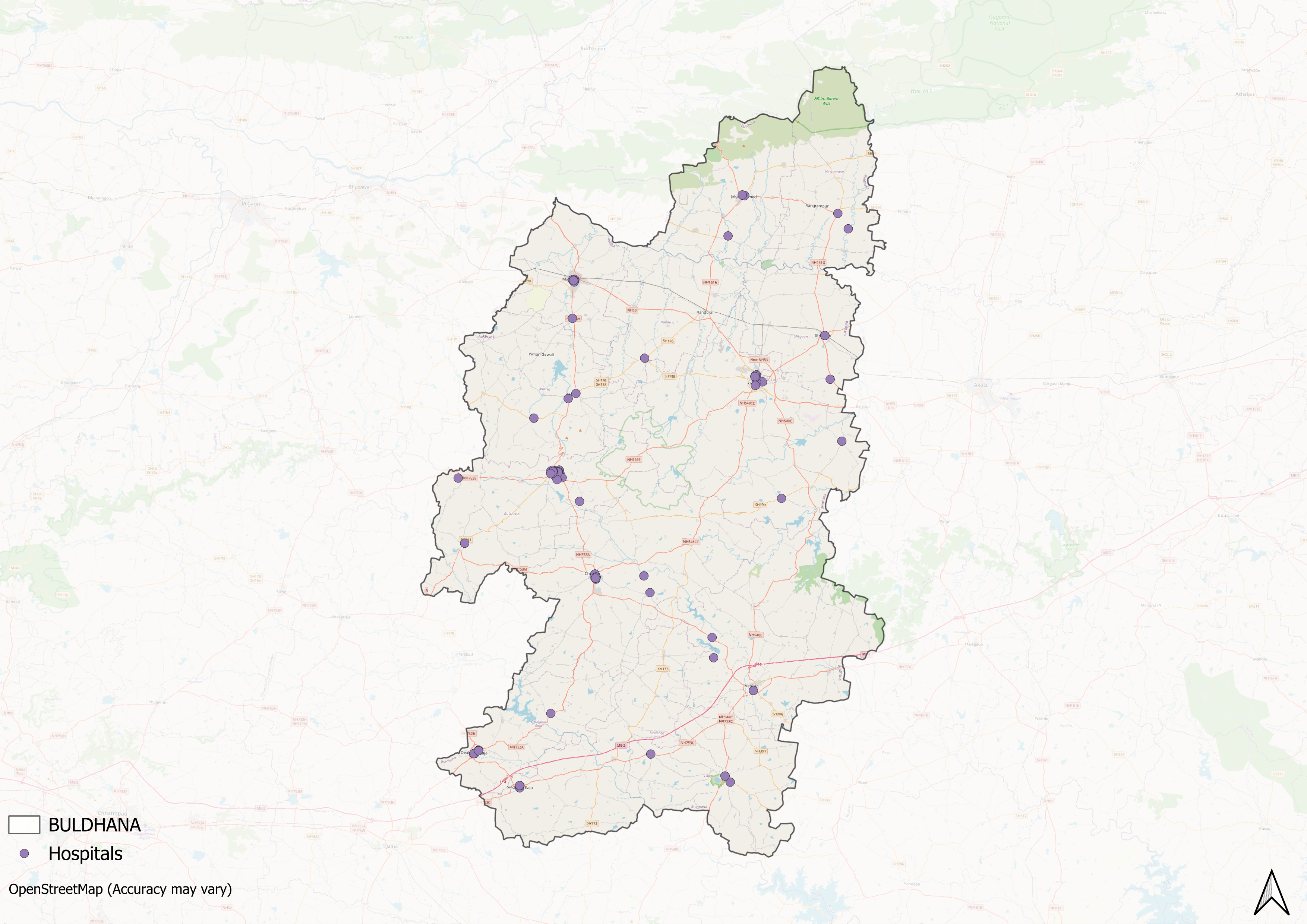
Healthcare Infrastructure
Much like other regions in India, Buldhana’s healthcare infrastructure follows a multi-tiered system that involves both public and private sectors. The public healthcare system is structured into primary, secondary, and tertiary levels. Primary care is provided through Sub Centres and Primary Health Centres (PHCs), secondary care is managed by Community Health Centres (CHCs) and Sub-District hospitals, while tertiary care, the highest level, is delivered through Medical Colleges and District Hospitals.
Supporting this structure is a network of Accredited Social Health Activists (ASHAs) who, as described by the National Health Mission, serve as “an interface between the community and the public health system.” Over time, this multi-layered healthcare model has been continuously shaped and refined by national healthcare policies and reforms to provide universal health coverage across regions. The district’s healthcare system has been shaped over time by various national health policies and reforms intended to improve access and coverage.
Among the oldest and most significant institutions is the District Civil Hospital, which continues to function as the main government healthcare facility.
![Buldhana District Hospital[1]](/media/statistic/images/maharashtra/buldhana/health/buldhana-district-hospital1-ea569c44.png)
As in many other districts, the early decades after independence saw public hospitals and dispensaries serving as the backbone of local healthcare. In the late 20th and early 21st centuries, many private hospitals and clinics also emerged. Many of these facilities have been established by local trusts, non-governmental organizations, and individual practitioners.
Medical Education & Research
Medical education and research form an important part of Buldhana’s healthcare system. As noted by Mathew Gerge (2023), medical institutions in India generally serve a “dual purpose” by training healthcare professionals and providing services to the local population. In Buldhana, both public and private institutions contribute to this sector.
Government Medical College
The Government Medical College, Buldhana, was established by the Government of Maharashtra on 14 July 2023. The college is affiliated with the Maharashtra University of Health Sciences, Nashik, and operates under the Directorate of Medical Education and Research, Government of Maharashtra. The District Civil Hospital and District Women’s Hospital, with a combined bed capacity of 420, are attached to the college to provide clinical training for students.
![Government Medical College, Buldhana[2]](/media/statistic/images/maharashtra/buldhana/health/government-medical-college-buldhana2-75dc291d.png)
Rajarshi Shahu College of Pharmacy
The Rajarshi Shahu College of Pharmacy in Buldhana was established in 2012 by the Dwarka Bahuudeshiya Gramin Vikas Foundation. The institution offers undergraduate (B.Pharm) and postgraduate (M.Pharm) programs across four disciplines. It operates with the objective of training professionals in the pharmaceutical sciences and contributing to the healthcare workforce in the region.
Graphs
Healthcare Facilities and Services
Morbidity and Mortality
Maternal and Newborn Health
Family Planning
Immunization
Nutrition
Sources
George, Mathew. 2023. "The Real Purpose of the Medical College." The Hinduhttps://www.thehindu.com/opinion/op-ed/the-r…
Government Medical College Buldhana. Home [GMC Buldhana]https://gmcbuldhana.org/
Home. Rajarshi Shahu College of Pharmacy.https://rscp.ac.in/
M Choksi, B. Patil et al. 2016. Health systems in India. Vol 36 (Suppl 3). Journal of Perinatology.https://pmc.ncbi.nlm.nih.gov/articles/PMC514…
Maharashtra State Gazetteers. 1976. Buldhana District Gazetteer. Gazetteer Department, Government of Maharashtra, Mumbai.https://gazetteers.maharashtra.gov.in/cultur…
National Health Mission (NHM). "About Accredited Social Health Activist (ASHA)." National Health Mission, Indiahttps://nhm.gov.in/index1.php?lang=1&level=1…
Last updated on 26 July 2025. Help us improve the information on this page by clicking on suggest edits or writing to us.