Contents
- Healthcare Infrastructure
- Medical Education & Research
- Government Medical College
- Age Old Practices & Remedies
- Hattibet
- Sailian Baba Dargah
- Graphs
- Healthcare Facilities and Services
- A. Public and Govt-Aided Medical Facilities
- B. Private Healthcare Facilities
- C. Approved vs Working Anganwadi
- D. Anganwadi Building Types
- E. Anganwadi Workers
- F. Patients in In-Patients Department
- G. Patients in Outpatients Department
- H. Outpatient-to-Inpatient Ratio
- I. Patients Treated in Public Facilities
- J. Operations Conducted
- K. Hysterectomies Performed
- L. Share of Households with Access to Health Amenities
- Morbidity and Mortality
- A. Reported Deaths
- B. Cause of Death
- C. Reported Child and Infant Deaths
- D. Reported Infant Deaths
- E. Select Causes of Infant Death
- F. Number of Children Diseased
- G. Population with High Blood Sugar
- H. Population with Very High Blood Sugar
- I. Population with Mildly Elevated Blood Pressure
- J. Population with Moderately or Severely High Hypertension
- K. Women Examined for Cancer
- L. Alcohol and Tobacco Consumption
- Maternal and Newborn Health
- A. Reported Deliveries
- B. Institutional Births: Public vs Private
- C. Home Births: Skilled vs Non-Skilled Attendants
- D. Live Birth Rate
- E. Still Birth Rate
- F. Maternal Deaths
- G. Registered Births
- H. C-section Deliveries: Public vs Private
- I. Institutional Deliveries through C-Section
- J. Deliveries through C-Section: Public vs Private Facilities
- K. Reported Abortions
- L. Medical Terminations of Pregnancy: Public vs Private
- M. MTPs in Public Institutions before and after 12 Weeks
- N. Average Out of Pocket Expenditure per Delivery in Public Health Facilities
- O. Registrations for Antenatal Care
- P. Antenatal Care Registrations Done in First Trimester
- Q. Iron Folic Acid Consumption Among Pregnant Women
- R. Access to Postnatal Care from Health Personnel Within 2 Days of Delivery
- S. Children Breastfed within One Hour of Birth
- T. Children (6-23 months) Receiving an Adequate Diet
- U. Sex Ratio at Birth
- V. Births Registered with Civil Authority
- W. Institutional Deliveries through C-section
- X. C-section Deliveries: Public vs Private
- Family Planning
- A. Population Using Family Planning Methods
- B. Usage Rate of Select Family Planning Methods
- C. Sterilizations Conducted (Public vs Private Facilities)
- D. Vasectomies
- E. Tubectomies
- F. Contraceptives Distributed
- G. IUD Insertions: Public vs Private
- H. Female Sterilization Rate
- I. Women’s Unmet Need for Family Planning
- J. Fertile Couples in Family Welfare Programs
- K. Family Welfare Centers
- L. Progress of Family Welfare Programs
- Immunization
- A. Vaccinations under the Maternal and Childcare Program
- B. Infants Given the Oral Polio Vaccine
- C. Infants Given the Bacillus Calmette Guerin (BCG) Vaccine
- D. Infants Given Hepatitis Vaccine (Birth Dose)
- E. Infants Given the Pentavalent Vaccines
- F. Infants Given the Measles or Measles Rubella Vaccines
- G. Infants Given the Rotavirus Vaccines
- H. Fully Immunized Children
- I. Adverse Effects of Immunization
- J. Percentage of Children Fully Immunized
- K. Vaccination Rate (Children Aged 12 to 23 months)
- L. Children Primarily Vaccinated in (Public vs Private Health Facilities)
- Nutrition
- A. Children with Nutritional Deficits or Excess
- B. Population Overweight or Obese
- C. Population with Low BMI
- D. Prevalence of Anaemia
- E. Moderately Anaemic Women
- F. Women with Severe Anaemia being Treated at an Institution
- G. Malnourishment Among Infants in Anganwadis
- Sources
LATUR
Health
Last updated on 26 July 2025. Help us improve the information on this page by clicking on suggest edits or writing to us.
Latur’s healthcare landscape, like many other regions across India, is shaped by a mix of indigenous and Western medical practices. For centuries, indigenous knowledge and treatments provided by practitioners such as hakims and vaidyas have formed the foundation of healthcare in the region. This long-standing relationship between communities and their natural environment played a key role in shaping the district’s early medical traditions. Over time, its landscape has gradually evolved with the introduction and expansion of more specialized medical services.
Healthcare Infrastructure
Similar to other regions in India, Latur’s healthcare infrastructure follows a multi-tiered system that involves both public and private sectors. The public healthcare system is structured into primary, secondary, and tertiary levels. Primary care is provided through Sub Centres and Primary Health Centres (PHCs), secondary care is managed by Community Health Centres (CHCs) and Sub-District hospitals, while tertiary care, the highest level, is delivered through Medical Colleges and District Hospitals.
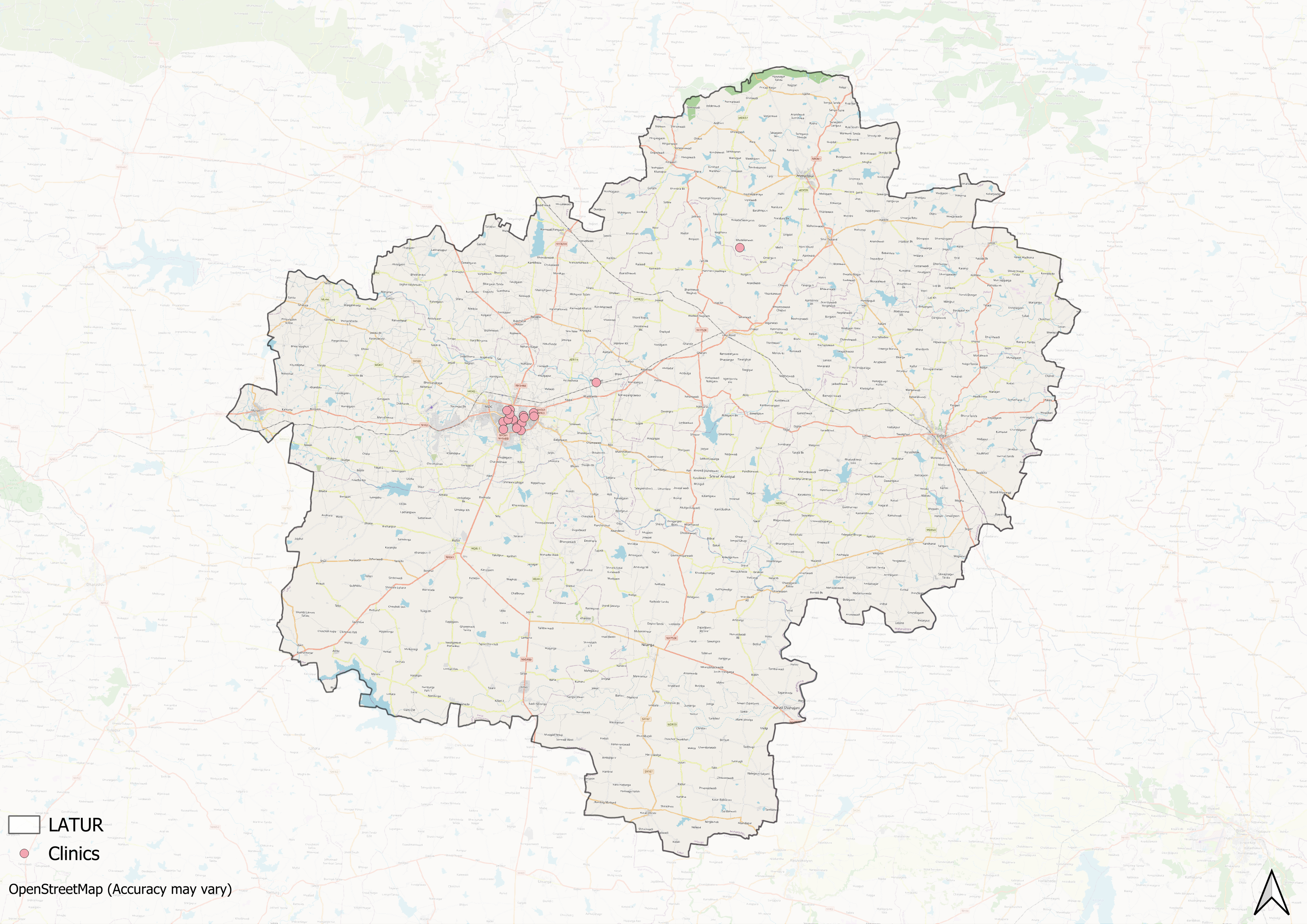
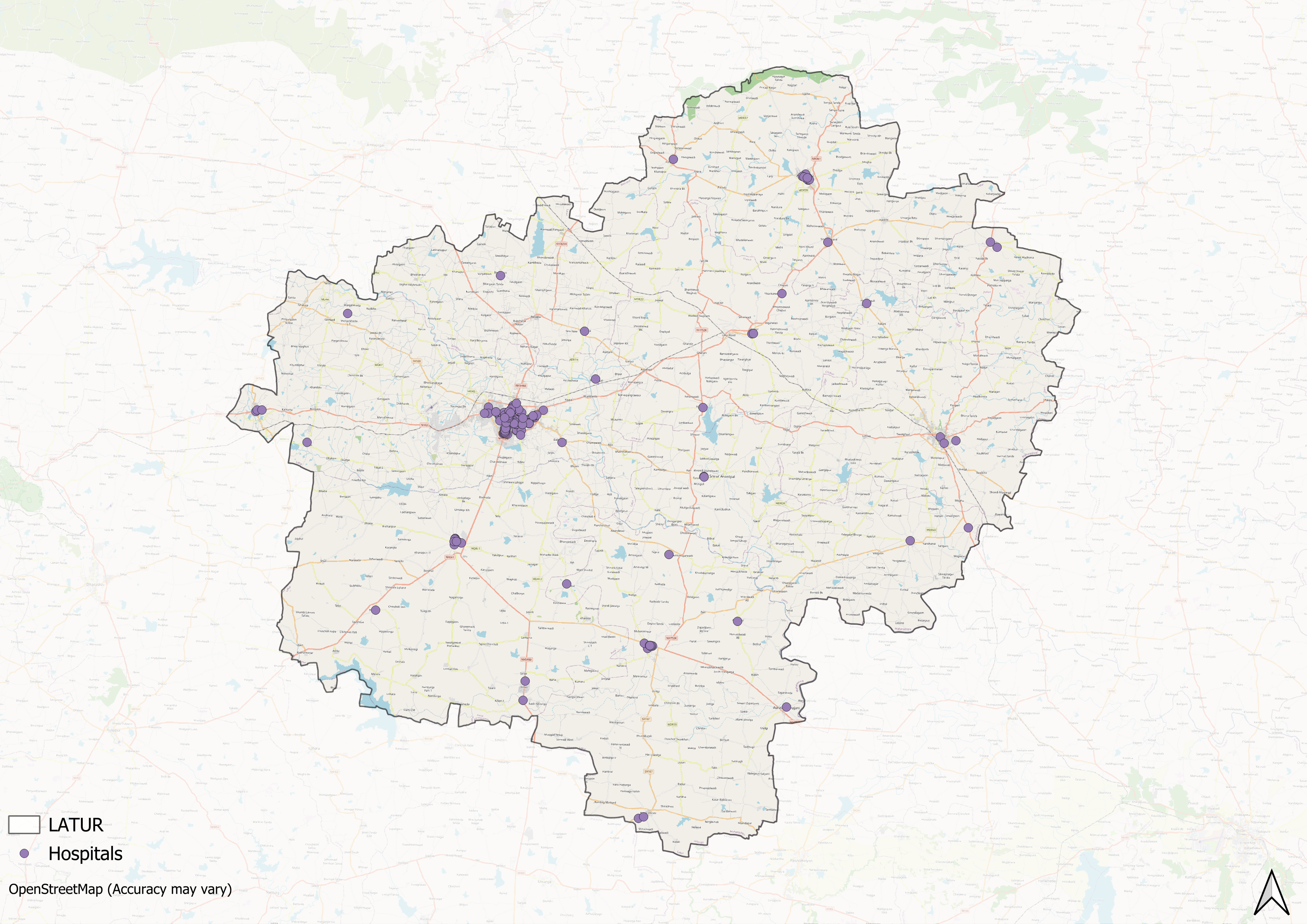
Supporting this structure is a network of Accredited Social Health Activists (ASHAs) who, as described by the National Health Mission, serve as “an interface between the community and the public health system.” Over time, this multi-layered healthcare model has been continuously shaped and refined by national healthcare policies and reforms to improve universal health coverage across regions.
In the 19th century, Latur was part of the princely state of Hyderabad. In 1905, it was integrated with surrounding areas and renamed Latur Tehsil under the larger Osmanabad district (now Dharashiv). Latur was declared an independent district in 1982, marking a shift in its administrative and developmental focus.
According to the Osmanabad district Gazetteer (1972), the region’s medical services during the early 20th century were centred around the Osmanabad General Hospital, while the Civil Hospital served as Latur’s main government facility. A government-run TB Chest Clinic was also set up to address rising tuberculosis cases at that time, showing an early effort to provide specialised care.
![Yashwantrao Chavan Hospital[1]](/media/statistic/images/maharashtra/latur/health/yashwantrao-chavan-hospital1-92f15cf6.png)
Over time, the public health infrastructure in the district began expanding. Additionally, in the 20th and 21st centuries, private facilities also started to emerge in Latur; with their establishment being driven by trusts, NGOs, and locals themselves.
A notable development during this time was the opening of the Yashwantrao Chavan Rural Hospital in August 1990 with an initial capacity of 200 beds. By 1995, the hospital expanded to 700 beds with additional specialisations. By 2004, it had also launched a comprehensive Ayurvedic Centre, reflecting a commitment to holistic health and marking a significant enhancement in the district’s rural healthcare capabilities.
Medical Education & Research
Medical education is an important part of Latur’s healthcare system, with institutions providing training for new healthcare professionals while delivering medical services to the district’s population. As Mathew Gerge (2023) notes, medical colleges in India often serve this “dual purpose” in regional healthcare.
Government Medical College
The Government Medical College, Latur, was established in 2002 under then Chief Minister Vilasrao Deshmukh to address the shortage of medical education facilities in Marathwada region.
![Government Medical College, Latur[2]](/media/statistic/images/maharashtra/latur/health/government-medical-college-latur2-e85613f1.png)
The college began by integrating the District Hospital (200 beds), Kasturba Gandhi Women’s Hospital (60 beds), and the Eye Hospital (60 beds), all managed by the Maharashtra Public Health Department. It is affiliated with the Maharashtra University of Health Sciences, Nashik.
Age Old Practices & Remedies
Historically, before the advent of Western health care systems or the three-tiered healthcare infrastructure that exists today, communities in Latur, like much of India, relied on indigenous knowledge and local remedies for their health needs. India has long been known for its pluralistic health traditions, where household treatments and plant-based remedies formed a significant part of daily life. Many of these practices have been passed down through generations, shaping family-level healthcare across rural and semi-urban areas.
Latur’s rural regions are especially noted for their diverse ethnobotanical traditions, where plants and herbs continue to be used for treating common ailments. In villages, local remedies draw on knowledge of roots, leaves, bark, and seeds.
Hattibet
Hattibet is a culturally significant site in Latur district, known both for its spiritual associations and for the diverse range of medicinal plants found in its hilly terrain. During the monsoon months of July and August, locals and visitors alike gather a variety of herbs reputed for their therapeutic properties.
![Hattibet Devarajan, Latur is known for its rich ethnobotanical heritage and traditional healing practices.[3]](/media/statistic/images/maharashtra/latur/health/hattibet-devarajan-latur-is-known-for-its-rich_UOiOJx9.png)
Among the plants commonly used in local remedies is Aconitum napellus (locally known as Vaachnag), whose root is employed to treat fever and joint pain.
![Vaachnag[4]](/media/statistic/images/maharashtra/latur/health/vaachnag4-e21dd469.png)
Another widely used preparation includes the leaves of Adhatoda vasica (known locally by various names such as Adusa, Arusa, and Basak) combined with the flowers of Hibiscus rosa-sinensis. The mixture is ground and consumed as a remedy for asthma. Such practices, in many ways, highlight the enduring presence of herbal medicine in the district’s healthcare traditions.
Sailian Baba Dargah
The Sailain Baba Dargah, located in Renapur, is associated with a historical figure believed to have migrated from Buldhana to Latur. Reputed for curing ailments through natural means, Sailain Baba remains a revered figure in local tradition. His samadhi lies within the dargah complex, which continues to attract devotees seeking relief and blessings for health.
Graphs
Healthcare Facilities and Services
Morbidity and Mortality
Maternal and Newborn Health
Family Planning
Immunization
Nutrition
Sources
AA Yelmate, Dr. SS Thonte.2018.“Ethnobotanical survey of plants on hattibet (Deverjan) district Latur Maharashtra.”.Vol. 7, no. 3.Journal of Pharmacognosy and Phytochemistry.https://www.phytojournal.com/archives/2018/vol7issue3/PartS/7-2-539-269.pdfhttps://www.phytojournal.com/archives/2018/v…
M Choksi, B. Patil et al. 2016.Health systems in India.Vol 36 (Suppl 3).Journal of Perinatology.https://pmc.ncbi.nlm.nih.gov/articles/PMC5144115/https://pmc.ncbi.nlm.nih.gov/articles/PMC514…
Maharashtra District Gazetteers. 1972.Osmanabad District. 1st ed. Government of Maharashtra.
MIT Pune.n.d. "Yashwantrao Chavan Rural Hospital, Latur." MIT Group of Institutions.https://mitpune.ac.in/colleges/hospitals/yashwantrao-chavan-rural-hospital-latur.htmlhttps://mitpune.ac.in/colleges/hospitals/yas…
National Health Mission (NHM). "About Accredited Social Health Activist (ASHA)." National Health Mission, India.https://nhm.gov.in/index1.php?lang=1&level=1&sublinkid=150&lid=226#:~:text=One%20of%20the%20key%20components,performing%20her%20spelled%20out%20roles.https://nhm.gov.in/index1.php?lang=1&level=1…
Vilasrao Deshmukh Government Medical College, Latur. "Brief History of VDGMC Latur." VDGMC Latur.https://www.vdgmclatur.org/briefhistory/https://www.vdgmclatur.org/briefhistory/
Vilasrao Deshmukh Government Medical College, Latur.n.d. "About Latur." VDGMC Latur. Accessed March 18, 2025.https://www.vdgmclatur.org/aboutlatur/https://www.vdgmclatur.org/aboutlatur/
Last updated on 26 July 2025. Help us improve the information on this page by clicking on suggest edits or writing to us.